- Abnormal Coagulogram
- Thrombocytopenia
- Platelet dysfunction
- Prothrombin complex Deficiency secondary to liver involvement
- Endothelial injury
- DIC and prolonged APTT
- Decreased fibrinogen level
- Increased level of fibrinogen degradation product (FDP)
- Increase level of D-Dimer
- Consumptive coagulopathy (activation of mononuclear phagocytes)
- Sequestration of platelet
2.1 Pathophysiology of Dengue Infection
exp date isn't null, but text field is
- Dengue virus, which has 4 distinct serotypes, i.e. DENV-1, DENV-2, DENV-3, DENV- 4 is transmitted by Aedes aegypti and Aedes albopictus to human.
- Infection with one serotype confers life long immunity to that serotype and cross immunity to other serotypes for 2-3 months only.
- The pathogenesis of dengue involves a complex interaction between virus and host factors, and remains incompletely understood. The immune system plays a key role in disease pathogenesis. Various mechanisms of severe disease have been suggested, including:
(a) Antibody-dependent enhancement or ADE,
(b) T-cell mediated immunopathology,
(c) Complement activation by virus-antibody complexes and
(d) Cytokine abundance.
- Non-neutralizing cross-reactive antibodies elicited in a primary infection bind virus in a secondary infection and then have a greater ability to infect Fc-receptor bearing cells (Monocytes, macro phages). This is called antibody-dependent enhancement (ADE), and potentially leads to an increased viral biomass, and therefore more chance of developing severe disease. In addition, there is evidence that ADE immunologically modulates infected cells in such a way that the micro environment becomes more supportive of DENV replication.
- The proliferation of activated memory T cells and the production of proinflammatory cytokines contribute to the development of plasma leak observe in severe dengue.
- Dengue infected monocytes act as antigen presenting cells (APCs) to induce release of lymphokines and other factors from activated T cells. Tumour Necrosis Factor-α, Interleukin (IL) IL-1b, IL-2, IL-6, IL-8, Interferon gamma (IFNɣ), RANTES etc. are the cytokines that are released from these cells.
- These cytokines along with complement breakdown products (C3a, C5a) activated in DHF/DSS, increases vascular permeability of vascular endothelial cells leading to DSS.
- Antibody dependent enhancement and inappropriate memory T-cell response are central to the pathogenesis of DHF/DSS.
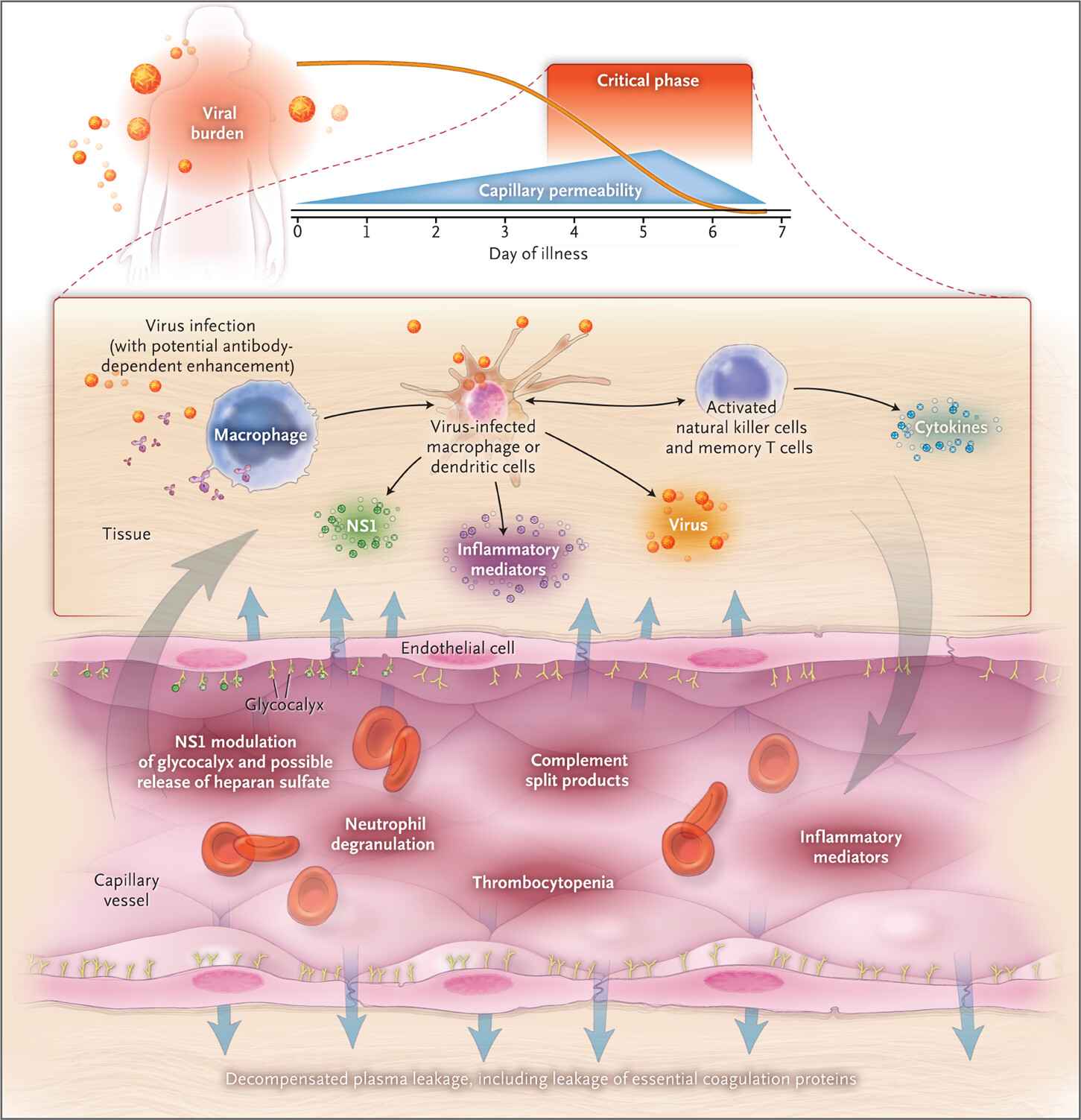
Figure 6 - Pathophysiology of dengue infection
Dengue: Review article, Simmons CP, Jeremy J. Farrar JJ, Vinh Chau NV,Wills B, N Engl J Med: April, 2012: 366:pp-1427)
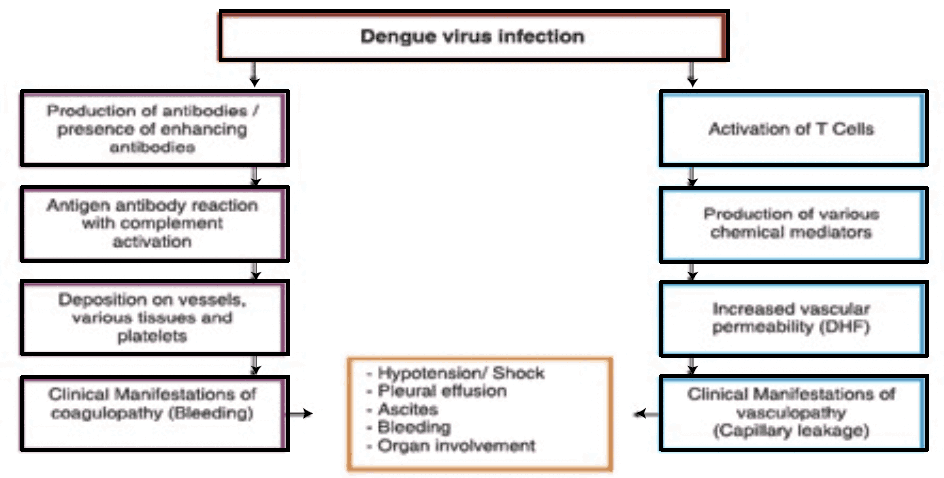
Figure 7 - Flow Chart of Pathophysiology of dengue infection
- Antibodies: Presence of enhancing and non-neutralizing antibodies.
- Age: susceptibility to DHF/DSS drops significantly after 12 yrs of age.
- Sex: female more often affected than male.
- Race: Caucasians more often affected than blacks.
- Sequence of Infection: Example, serotype 1 followed by serotype 2 is more dangerous than serotype 4 followed by serotype 2.
- Infecting Serotype: Type 3 is more dangerous than others.
- Infecting Genotype: Asian type 2 causes DHF/DSS while American type is not responsible for the illness.